 New
New 
Did you know that up to 10% of the population will experience a seizure during their lifetime (WHO 2023)?
What would you do if someone had a seizure in front of you? Would you know how to describe what type of seizure it was? Would you know how to help them?
What is a Seizure?
A seizure occurs when there is a disturbance within the brain caused by sudden, abnormal electrical and neuronal activity (Epilepsy Foundation 2019).
An individual will be diagnosed with epilepsy if they experience two or more seizures that are unprovoked and not known to be caused by a medical condition (WHO 2023).
Types of Seizures
There are three major groups of seizures: generalised onset, focal onset, and unknown onset (Epilepsy Action Australia 2023).
Generalised onset seizures involve both hemispheres of the brain at once, whereas focal onset seizures involve electrical disturbances in one specific area of the brain, which may then spread to other areas. Unknown onset seizures are unable to be classified as generalised onset or focal onset, but this might change if more information becomes available. It is only in rare cases that the type of seizure remains unable to be determined, usually because there is not enough information available or the symptoms are abnormal (Epilepsy Action Australia 2023).
Seizures may have motor or non-motor symptoms (Epilepsy Action Australia 2023).
Focal Onset Seizures
Focal onset seizures may be subtle and unnoticeable or present as unusual behaviours. They may be mistaken for daydreaming or being intoxicated. About 60% of people with epilepsy experience focal onset seizures (Epilepsy Action Australia 2023).
There are two further subgroups of focal onset seizures:
- Focal aware seizures, where the person retains complete awareness of their surroundings. However, they may be unable to speak or respond. These seizures may only last for a short amount of time.
- Focal impaired seizures, where the person experiences impaired awareness and may be confused, vague or disoriented.
(Epilepsy Action Australia 2023)
Generalised Onset Seizures
Because generalised seizures are the result of abnormal electrical activity in both hemispheres of the brain, the individual may lose consciousness at the onset of the seizure. Awareness is almost always affected (Epilepsy Action Australia 2023).
Types of generalised onset seizures include:
- Absence seizures, which involve a sudden impairment of awareness. The person may stare into space, daydream or perform subtle movements like blinking or smacking their lips.
- Tonic seizures, which cause muscles (usually in the back, arms and legs) to stiffen. If the person is sitting or standing, they may fall over.
- Clonic seizures, which cause muscles (usually in the neck, face and arms) to jerk repeatedly or rhythmically.
- Atonic seizures, which are characterised by a brief, sudden loss of muscle tone. The person may fall over or experience a sudden head nod if they are sitting.
- Myoclonic seizures, which are sudden, singular jerks of a muscle or group of muscles. They are often very brief.
- Tonic-clonic seizures, which involve both tonic and clonic phases. The person may lose consciousness, experience stiffening or shaking of the body, lose bladder control or bite their tongue.
(Epilepsy Action Australia 2023; Mayo Clinic 2023)
Signs of a Seizure
A patient having a seizure might:
- Cry out
- Fall onto the ground
- Briefly stiffen and go rigid
- Experience rhythmic jerking muscular movements
- Appear pale, with blue lips
- Produce excessive saliva
- Bite their tongue or cheek, causing bloody saliva
- Lose bladder or bowel control
- Be tired, confused or agitated after the seizure.
(St John 2022)
Nursing Management of Someone Having a Seizure
Patient safety is one of the main considerations during seizure activity. It is important to remember DRSABCD:
- Danger
- Response
- Send for help
- Airway
- Breathing
- CPR
- Defibrillation.
(St John 2022)
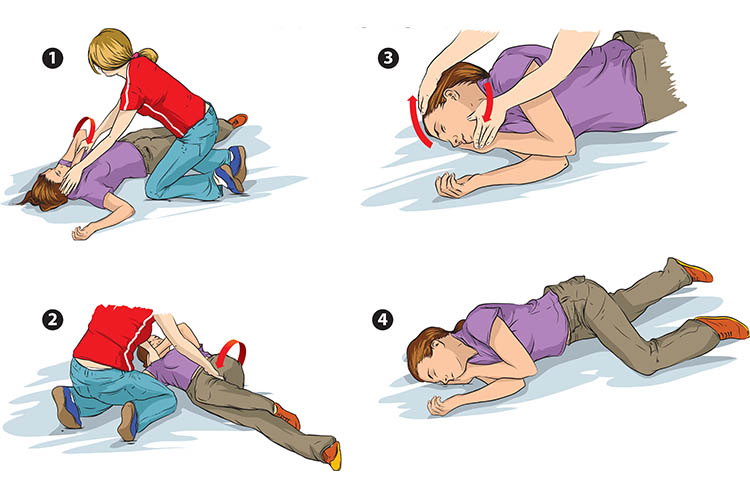
The nurse must stay with the patient and call for help. It is important to time the seizure and note its characteristics. Protection must be given to the patient’s head, especially with any convulsive movements occurring that may injure the patient. You can protect the patient from harming themselves by placing something soft under their head and shoulders. The surrounding area must be made clear to decrease the risk of injury, however, do not try to physically restrict the movement of the patient’s limbs, as this can cause musculoskeletal damage. Do not put anything in the patient’s mouth or attempt to move them (St John 2022).
As soon as you are able to do so, roll the patient onto their side in the recovery position to prevent aspiration due to excessive saliva production and ensure their airway remains patent. If the patient has vomited or has food or fluids in their mouth, it is crucial to do this immediately (St John 2022).
Suction and oxygen must be available. Monitoring of vital signs is imperative, especially respiratory function.
Following the seizure, manage any resulting injuries. Continue to monitor the patient’s airway, using suction as needed, and do not disturb the patient if they fall asleep. When they wake, calmly tell them where they are and that they are safe. Provide reassurance, as this can understandably be quite distressing for the patient (St John 2022).
Frequent monitoring of vital signs and neurological observations will need to be performed in order to monitor the patient’s condition.
Note: This article is intended as a refresher and should not replace best-practice care. Always refer to your organisation's policy on seizure first aid.
Topics
References
- Epilepsy Action Australia 2023, Seizure Types and Classification, Epilepsy Action Australia, viewed 29 November 2023, https://www.epilepsy.org.au/about-epilepsy/understanding-epilepsy/seizure-types-and-classification/
- Epilepsy Foundation 2019, What is a Seizure?, Epilepsy Foundation, viewed 29 November 2023, https://epilepsyfoundation.org.au/understanding-epilepsy/seizures/what-is-a-seizure/
- Mayo Clinic 2023, Seizures, Mayo Clinic, viewed 29 November 2023, https://www.mayoclinic.org/diseases-conditions/seizure/symptoms-causes/syc-20365711
- St John 2022, First Aid Fact Sheet: Epileptic Seizure, St John Ambulance Australia, viewed 29 November 2023, https://stjohn.org.au/assets/uploads/fact%20sheets/english/Fact%20sheets_epileptic%20seizure.pdf
- World Health Organisation 2023, Epilepsy, WHO, viewed 29 November 2023, https://www.who.int/news-room/fact-sheets/detail/epilepsy